aspirin exacerbated respiratory disease
- related: Pulmonology
- tags: #pulmonology
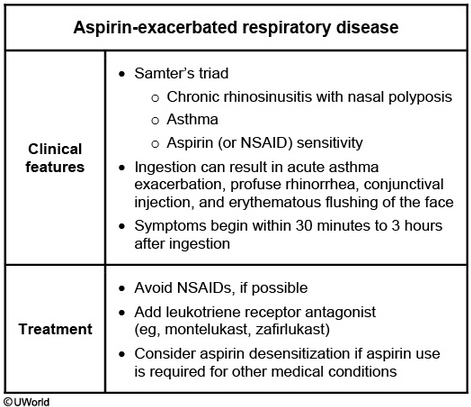
This patient’s presentation is consistent with aspirin-exacerbated respiratory disease (AERD), as summarized in the table. AERD affects up to 20% of adult asthmatics and usually presents with the classic triad of chronic rhinosinusitis with polyposis, asthma, and aspirin (or NSAID) sensitivity. Patients usually develop refractory rhinitis in their 30s followed by chronic rhinosinusitis with anosmia and nasal polyposis. The rhinosinusitis progresses to lower-airway inflammation, resulting in asthma. Aspirin and NSAID sensitivity develops during this progression. NSAIDs can induce life-threatening asthma, nasal and/or ocular symptoms, and facial flushing or erythema.
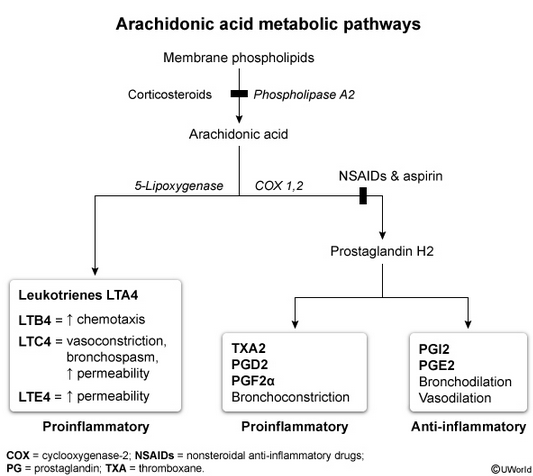
The reaction is not an IgE-mediated allergic response but is likely a shift in the arachidonic acid metabolic pathway causing excessive leukotriene production. Diagnosis is made clinically with history of aspirin or NSAID reaction. Treatment involves optimal asthma therapy, surgery for chronic rhinosinusitis, and avoidance of NSAIDs or aspirin. Current guidelines also recommend a leukotriene receptor antagonist (e.g., montelukast) to improve pulmonary and sinus symptoms. Aspirin desensitization is considered in patients refractory to therapy or who require aspirin/NSAIDs for other chronic conditions (e.g., CAD, chronic headaches).
Anti-IgE therapy is beneficial in IgE-mediated conditions such as moderate to severe asthma with perennial allergies. However, AERD is not IgE mediated.
Adding tiotropium can improve symptoms and lung function in uncontrolled asthmatics, but leukotriene antagonists are preferred in patients with AERD.